Gender & Drug Response Checker
Select your biological sex and a medication class to view potential physiological risks and dosage insights based on current research.
General Metabolic Insights
InformationalRisk Summary: Women generally process drugs differently due to distinct physiological markers.
The Biological Why: Key factors include Cytochrome P450 enzyme activity levels and body composition ratios (fat vs. muscle mass).
Clinical Consideration: Understanding these baseline differences is the first step toward safer prescription practices.
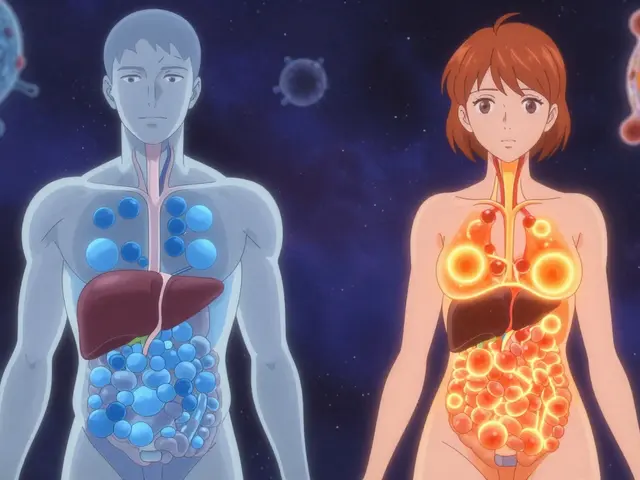
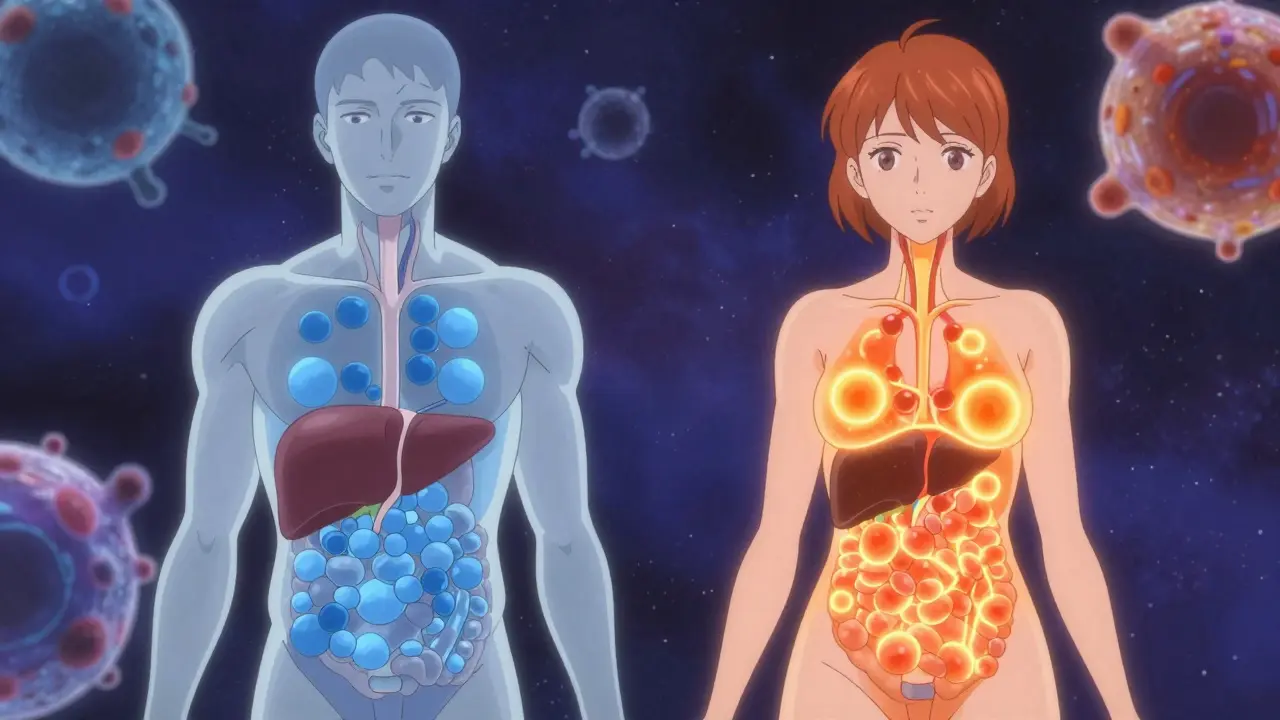
Did you know that women experience adverse drug reactions nearly twice as often as men? Statistics show an 80 to 90 percent higher incidence rate among females compared to males. This isn't just anecdotal evidence; it's a documented reality backed by decades of safety monitoring. Yet, walk into any pharmacy, grab a standard prescription, and read the label. Chances are, you won't find specific instructions for your gender. For years, medical science has operated on a "default male" assumption, treating female physiology as a minor variation rather than a fundamental difference.
The implications are serious. We aren't talking about mild discomforts here. The cost of these oversights reaches into the billions annually in wasted healthcare resources. More importantly, individuals suffer through unnecessary toxicity or ineffective treatment because their biology was never accounted for. As regulations tighten and science finally catches up, understanding these distinctions becomes crucial for patient safety. Your body processes chemicals differently depending on your sex, and ignoring this leads to real harm.
The Biological Blueprint
At the core of this issue lies human biology. While genetics provide the blueprint, factors like enzyme activity and body composition dictate how your system handles introduced substances. When a medication enters your bloodstream, it doesn't just float there waiting to work. Your body treats it as a foreign invader that needs processing and removal. This is where the divergence starts.
Consider the liver. It houses the primary filtration team, including a group of proteins known as cytochrome P450 enzymes. Specifically, the CYP3A4 enzyme is responsible for metabolizing about 50 percent of all common prescription drugs. Research indicates that women generally have significantly lower activity levels of this enzyme compared to men. With less enzymatic power available, the same dose of medication stays in a woman's system longer. This accumulation creates a perfect storm for side effects.
Then there is the matter of physical composition. Men typically carry less body fat than women-averaging around 16 to 18 percent versus 28 percent in women. Fat-soluble medications, those designed to dissolve in lipids rather than water, get trapped in adipose tissue. In women, these drugs have more storage space, meaning they linger longer before being cleared. Drugs like diazepam can remain in the system 20 to 30 percent longer due to this simple physical variance. Add to this slower kidney clearance rates, and the picture of heightened risk becomes undeniable.
Cytochrome P450 enzymes are critical liver proteins responsible for drug metabolism, with significant variations observed between sexes that directly impact dosage tolerance and side effect frequency.Hormonal Influences
Beyond static physical traits, hormonal fluctuations add a layer of dynamic complexity. A woman's hormonal profile is not static; it shifts constantly throughout the month. These shifts alter the very mechanisms used to break down drugs. Estrogen and progesterone interact with liver enzymes, sometimes inhibiting them, sometimes speeding them up.
For example, during different phases of the menstrual cycle, the ability to process certain medications can fluctuate by up to 30 percent. Imagine taking the same pill daily but having your body absorb and eliminate it at different speeds each week. This unpredictability is often misdiagnosed as non-compliance or worsening illness. Furthermore, external hormonal interventions like oral contraceptives actively compete with other medications for metabolic pathways. Lamotrigine, a common anti-seizure medication, loses up to 60 percent of its effectiveness when combined with birth control pills, necessitating massive dose adjustments to prevent seizures.

Medications Where Gender Matters Most
While these biological rules apply broadly, specific drug classes show dramatic discrepancies. Identifying these helps patients advocate for safer prescriptions.
| Medication Class | Common Examples | Risk Factor for Women | Risk Factor for Men |
|---|---|---|---|
| Sedative-Hypnotics | Zolpidem (Ambien) | Slower metabolism leading to next-day impairment; FDA mandated 50% dose reduction | Faster clearance; standard dose usually safe |
| Antidepressants | SSRIs (Sertraline, Fluoxetine) | Higher rates of nausea, dizziness, sexual dysfunction | Lower reporting of acute GI issues |
| Cardiac Agents | Digoxin | Higher blood concentrations at standard doses; increased toxicity risk | Larger volume of distribution; lower concentration |
| Antipsychotics | Haloperidol | Higher risk of QT prolongation (heart rhythm issues) | Lower incidence of cardiac rhythm disturbances |
Zolpidem provides a classic case study in regulatory evolution. Evidence emerged in the early 1990s showing women metabolized the sleep aid much slower than men. Despite this, labeling didn't change until 2013. By that time, many women had suffered morning grogginess and potential cognitive impairment because the "standard" dose was effectively an overdose for female physiology. Similarly, digoxin, used to support heart failure, shows that women have significantly higher drug concentrations at standard weights, raising the bar for toxicity without changing the dose.
Historical Gaps in Research
Why does this discrepancy persist? To understand the present, we must look back at the 1970s and 80s. During this era, the Food and Drug Administration recommended excluding women of childbearing age from early-phase clinical trials. The logic was intended to protect the fetus from experimental drugs. However, the outcome was unintentional. Medical researchers ended up testing almost exclusively on men, establishing "normal" reaction baselines based solely on male biology.
Clinical Trials are research studies performed on humans to evaluate the safety and efficacy of medical treatments, historically biased toward male subjects which created current dosing gaps.It took decades to correct course. The 1993 NIH Revitalization Act eventually forced inclusion, yet implementation lagged. Even today, while women comprise roughly half of trial participants, fewer than one in ten studies actually analyzes whether men and women respond differently. This lack of analysis means doctors are often flying blind, relying on population averages that favor male physiology.

Navigating Your Health Journey
Patients shouldn't wait for policy to trickle down to their prescription pad. Awareness is the first line of defense. If you notice standard doses leave you feeling worse or unwell, speak up immediately. Documenting side effects allows clinicians to adjust therapy quickly. Asking about sex-specific data can also be empowering. Questions like, "Do I need a lower dose based on my gender?" force a deeper review of the protocol.
Doctors are increasingly aware of these gaps, but busy clinics often rely on automated dispensing systems that default to average doses. Bringing information to appointments helps bridge that knowledge gap. Reporting adverse events is another vital step. When women report reactions specifically noting their sex, it adds pressure for manufacturers to update labels with better warnings.
The Future of Dosage
We are moving toward a future where precision medicine accounts for these variables. AI-driven algorithms are currently being tested to predict individual metabolism rates based on sex, weight, and genetic markers. The FDA has launched roadmaps aimed at integrating these considerations across all regulatory activities by 2026. Legislative efforts, such as the proposed Fair Trials for Women Act, seek to mandate sex-specific recommendations for all new drug approvals.
While the landscape is improving, the burden remains partially on the individual to recognize that "average" does not equal "optimal." Understanding that your biology dictates your drug response is the first step in demanding care tailored to your unique physiology.
Why do women have more side effects than men?
Women process drugs differently due to smaller muscle mass, higher body fat percentage, and lower liver enzyme activity (like CYP3A4). These biological factors cause medications to stay in the system longer, increasing the likelihood of adverse reactions.
Does birth control affect medication side effects?
Yes, hormonal contraceptives can interact with liver enzymes, potentially reducing the effectiveness of certain drugs like lamotrigine or altering how antidepressants are processed, requiring dose adjustments.
Are drug doses adjusted for women?
Only for a small number of medications, such as zolpidem (Ambien). Historically, most drug labels provide a single standard dose, though this practice is changing slowly as research highlights the need for sex-specific dosing.
What should I tell my doctor about side effects?
If you experience persistent symptoms, inform your doctor immediately. Ask if gender differences might explain the severity and request a review of the dosing strategy to see if a lower starting dose is safer for you.
Do men also experience gender-specific side effects?
Men do face unique risks, such as higher rates of urinary retention with anticholinergic drugs and greater incidence of medication-induced sexual dysfunction, proving that sex-based physiology matters for everyone.