
For years, parents were told to keep peanuts away from babies. Delaying peanut exposure was seen as the safest way to prevent allergies. But that advice turned out to be wrong - and it cost children their health. Today, we know the opposite is true: introducing peanut early can stop peanut allergy before it starts. This isn’t theory. It’s science backed by major studies, updated guidelines, and real-world results.
What Changed? The LEAP Study That Rewrote the Rules
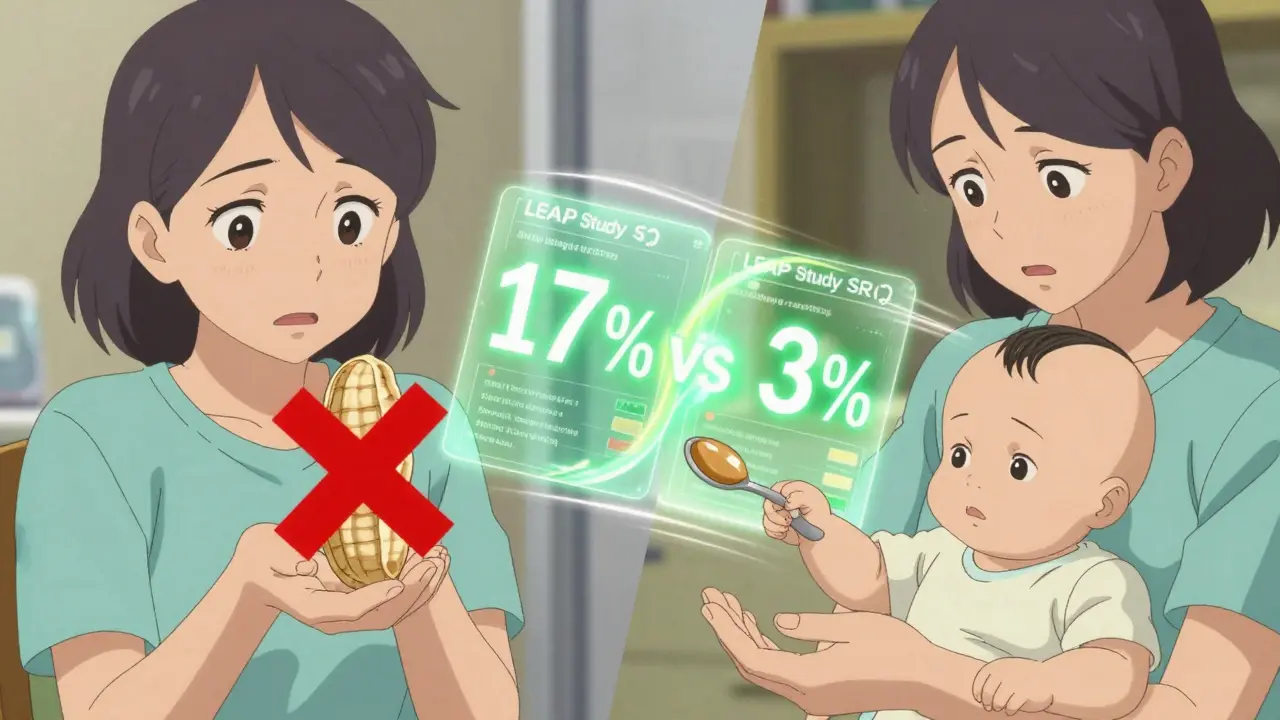
In 2015, the Learning Early About Peanut Allergy (LEAP) study shook the medical world. Led by Dr. Gideon Lack at King’s College London, researchers tracked over 600 high-risk infants - those with severe eczema or egg allergy. Half were given peanut-containing foods regularly starting at 4 to 6 months. The other half avoided peanuts entirely until age 5.
The results were startling. Among children who avoided peanuts, 17% developed peanut allergy by age 5. Among those who ate peanut early? Just 3%. That’s an 80% drop in allergy risk. This wasn’t a small effect. It was a game-changer.
Before LEAP, the American Academy of Pediatrics recommended waiting until age 2 or 3 to introduce peanuts, especially for babies with eczema or family allergies. After LEAP, the National Institute of Allergy and Infectious Diseases (NIAID) released new guidelines in 2017. These guidelines, endorsed by over 26 medical groups, completely flipped the script.
How to Introduce Peanut Based on Risk Level
Not all babies are the same. The current NIAID guidelines divide infants into three risk groups. Your baby’s risk level determines how and when to start.
- High-risk infants - those with severe eczema or egg allergy - should be evaluated by a doctor or allergist between 4 and 6 months. If allergy tests come back negative, introduce 2 grams of peanut protein three times a week. That’s about 2 teaspoons of smooth peanut butter, mixed into warm water, breast milk, or pureed fruit. The first dose should be given under medical supervision.
- Moderate-risk infants - those with mild to moderate eczema - can start peanut around 6 months at home. No testing is needed. Just mix smooth peanut butter into food and watch for reactions.
- Low-risk infants - no eczema or food allergies - can have peanut introduced anytime after starting solids, usually around 6 months. No special steps needed.
Timing matters. The best window is before 6 months. A 2023 analysis of LEAP and the EAT study found that babies who started peanut before 6 months had up to a 98% lower chance of developing allergy - if they stuck to the plan. Even those with severe eczema saw a 67% reduction. Delaying beyond 6 months cuts the benefit significantly.
Safe Ways to Give Peanut to Babies
You can’t just hand a baby a handful of peanuts. Whole peanuts are a choking hazard. Even chunky peanut butter is too thick and sticky for infants.
Here’s what works:
- Smooth peanut butter mixed with 2-3 tablespoons of warm water, breast milk, or formula to make a thin paste.
- Stirred into infant cereal, applesauce, or mashed banana.
- Peanut puff snacks like Bamba - a soft, dissolvable snack popular in Israel and now available in the U.S.
- Specialized peanut powder products designed for infants, now sold in pharmacies and baby stores.
Start with a small amount - about 1/4 teaspoon - and wait 10 minutes. Watch for signs like hives, vomiting, or trouble breathing. If nothing happens, give the rest. Do this three times a week. Consistency is key. Skipping days reduces the protective effect.
Oral Immunotherapy (OIT) Is Not Prevention - It’s Treatment
Many people confuse early introduction with oral immunotherapy (OIT). They’re not the same thing.
Early introduction is for babies who don’t have peanut allergy yet. It’s prevention. OIT is for children who already have a confirmed peanut allergy. In OIT, kids eat tiny, gradually increasing amounts of peanut under medical supervision to build tolerance. It doesn’t cure the allergy - it just helps reduce the risk of a severe reaction if they accidentally eat peanut.
OIT is not a home experiment. It requires a specialist, careful monitoring, and carries risks. It’s not recommended for prevention. The goal of early introduction is to avoid needing OIT altogether.
Why So Many Parents Still Wait
Despite clear guidelines, only about 39% of high-risk infants get peanut introduced early, according to a 2022 study in Pediatrics. Why?
- Fear of reactions - parents worry about anaphylaxis, especially if their baby has eczema.
- Confusion - many pediatricians still give outdated advice. A 2023 survey found only 54% of pediatricians knew the current guidelines.
- Access - seeing an allergist isn’t easy. Wait times can be months long.
- Cultural and racial gaps - Black and Hispanic infants are 22% less likely to get early peanut exposure than White infants, according to a 2023 study. This contributes to ongoing disparities in allergy rates.
It’s not just about knowledge. It’s about support. Parents need clear instructions, safe product options, and reassurance. Pediatricians need training. Health systems need better systems to track and remind families.
What the Data Shows: Real Results Since 2017
The impact is already visible. In the U.S., peanut allergy rates among children dropped from 2.2% in 2015 to 1.6% in 2023, according to Food Allergy Research & Education (FARE). That’s about 300,000 fewer children with peanut allergy.
And it’s not just numbers. Long-term follow-up from the LEAP study showed that the protection lasted - even after kids stopped eating peanut for a full year. That suggests early exposure doesn’t just mask the allergy. It trains the immune system to accept peanut as safe.
Australia saw similar results. After changing their guidelines in 2016 to recommend early introduction, peanut allergy dropped fivefold in babies introduced around 6 months compared to those introduced after 10 months.
What’s Next? The Future of Allergy Prevention
Research is moving beyond peanut. The EAT study showed that introducing multiple allergens - egg, milk, tree nuts - early can reduce the risk of multiple food allergies. The NIAID-funded PRESTO trial, expected to finish in 2026, is testing whether even earlier exposure - at 3 months - works better for the highest-risk babies.
Scientists are also studying how skin health affects allergy risk. Babies with cracked, inflamed skin (like severe eczema) absorb peanut proteins through their skin, which can trigger allergy. That’s why introducing peanut by mouth early helps - it teaches the gut immune system to respond safely.
Meanwhile, the market is adapting. Peanut puff snacks, spoonable peanut butter pouches, and medical-grade peanut powders are now widely available. Insurance coverage for allergist visits is slowly improving. But progress is uneven.
What Parents Should Do Now
If you’re expecting or have a baby under 12 months:
- Check your baby’s risk level: Do they have severe eczema or egg allergy? If yes, talk to your pediatrician by 3-4 months.
- Don’t wait. If your baby is 4-6 months old and developmentally ready for solids, start peanut now - even if you haven’t talked to a doctor yet.
- Use smooth peanut butter or peanut puff snacks. Never give whole peanuts or chunky butter.
- Give peanut 3 times a week. Don’t skip. Consistency beats perfection.
- Watch for reactions. If you see hives, swelling, vomiting, or trouble breathing, call 911.
- Keep going. Even if your baby seems fine, keep offering peanut regularly. The protection fades without regular exposure.
It’s not about being perfect. It’s about being timely. The window for prevention is narrow - and closing fast. Waiting for "the right time" might mean missing it entirely.
Can I introduce peanut if my baby has eczema?
Yes - and you should. Babies with eczema are at higher risk for peanut allergy. The NIAID guidelines recommend evaluating high-risk infants (severe eczema) with a doctor or allergist before starting. If testing is negative, introduce peanut between 4 and 6 months. For mild to moderate eczema, you can start at home around 6 months without testing.
Is peanut butter safe for babies?
Only smooth peanut butter, thinned with water, breast milk, or formula. Never give chunky peanut butter, whole peanuts, or peanut pieces - they’re choking hazards. Mix 2 teaspoons of smooth peanut butter with 2-3 tablespoons of liquid to make a runny paste. Start with a small amount and watch for reactions.
What if my baby has a reaction to peanut?
Stop giving peanut immediately. If the reaction is mild - like a few hives - call your pediatrician. If there’s swelling, vomiting, trouble breathing, or the baby seems unwell, call 911 or go to the ER. This could be anaphylaxis. Do not wait. Even if it’s the first time, treat it seriously. Follow up with an allergist to confirm if it’s a true allergy.
Do I need to test my baby before giving peanut?
Only if your baby is high-risk - meaning severe eczema or egg allergy. In that case, your doctor may recommend a skin prick test or blood test. If the test is negative, you can start peanut at home. For moderate or low-risk babies, no testing is needed. Just start with a small amount at home.
Can I prevent peanut allergy by avoiding it during pregnancy?
No. Studies have found no benefit to avoiding peanuts during pregnancy or breastfeeding. In fact, avoiding peanut during pregnancy doesn’t lower allergy risk. The only proven method is introducing peanut to the baby early - between 4 and 6 months. Focus on your baby’s diet, not your own.
How long do I need to keep giving peanut to my baby?
Until at least age 5. The research shows that regular exposure - at least 3 times a week - is needed to maintain protection. Stopping too soon can undo the benefit. Once your child is eating peanut regularly as part of their diet, you don’t need to measure it precisely. Just make sure peanut is a normal part of their meals.
Final Thought: Prevention Is Possible
Peanut allergy used to feel inevitable - especially if your child had eczema or a family history. Now, we know it’s not. The science is clear: early, consistent exposure saves lives. It’s not risky. It’s the safest thing you can do. The hardest part isn’t the method - it’s overcoming fear. But fear is based on old advice. The new advice? It works.

so like... uhh peanut butter? for babies? lol i mean i get the science but what if they choke? my cousin's kid almost died on a grape and now i just give em mashed bananas forever
Let me be perfectly clear: delaying peanut exposure was not just misguided-it was a catastrophic failure of medical orthodoxy rooted in fear, not evidence. The LEAP study didn’t just ‘change guidelines’-it exposed a systemic collapse in pediatric risk aversion that prioritized parental anxiety over infant immunity. This isn’t ‘new advice.’ It’s the reclamation of science from the clutches of alarmist pedagogy. And if you’re still waiting for ‘the right time,’ you’re not being cautious-you’re complicit in preventable disease.
This is such an important topic! I’m a pediatric nurse in India and I’ve seen so many parents terrified of introducing peanuts-even when their baby has no eczema or allergies. We’ve started handing out simple printed guides with images of smooth peanut butter mixed in yogurt or cereal. Small changes make a huge difference. Consistency matters more than perfection. Just keep offering it, gently, regularly. Your baby’s immune system will thank you.
My daughter was high-risk-severe eczema from birth. We did the skin test, it came back negative, and we started with 1/4 tsp of peanut butter mixed into her oatmeal at 4 months. Three times a week. No drama. No reactions. Now she’s 2 and eats peanut butter sandwiches like a champ. The fear was way worse than the reality. Just follow the steps. You got this.
ok but what if the study was funded by peanut companies? i mean seriously, who benefits? also, why did the aap wait so long to change? maybe they were just lazy? also, i read somewhere that 80% reduction is only for high-risk, not everyone, so why are we generalizing? and also, what about the kids who still got allergies despite early exposure? they exist. why dont we talk about them?
Oh, so now we’re all supposed to be little immunologists before we even change our baby’s diaper? Brilliant. Let’s just hand out syringes with peanut slurry and call it ‘parenting.’ Meanwhile, the real issue is that pediatricians are still stuck in 2008 and parents are left to Google their way through anaphylaxis. Bravo, science. You turned parenting into a high-stakes game of Russian roulette with a spoon.
There’s a metaphysical irony here, isn’t there? We’ve weaponized food to test the fragility of the human immune system-turning nourishment into a ritual of existential risk. Early exposure isn’t just medical-it’s a symbolic surrender to chaos. We no longer protect our children from the world… we force them to digest it. And in that act, we confess: we never had control to begin with.
peanut butter at 4 months? sounds like a bad idea tbh. my kid got sick once and now i just avoid everything. also why is everyone so sure? science changes all the time. remember when eggs were bad?
I want to say thank you to whoever wrote this. I’m a single mom of a baby with moderate eczema, and I was paralyzed with fear. I read this at 2 a.m., cried, and the next day I mixed smooth peanut butter into her applesauce. She loved it. No reaction. I’ve been doing it three times a week for six weeks now. It’s not about being perfect-it’s about showing up. You gave me the courage to try. And honestly? That’s worth more than any guideline.
So now we’re supposed to feed our babies peanut butter because some study said so? What’s next? Injecting them with shellfish at birth? This is just another trend pushed by overzealous doctors who think they know better than moms. My grandma never gave peanuts until age 5 and I turned out fine. We don’t need science to tell us to be careful.
I’m from South Africa and I’ve seen this play out in my community-so many Black and Brown families told to wait, scared, confused, left behind. This isn’t just science. It’s justice. When we give parents clear, simple, culturally relevant tools-like peanut puff snacks in local clinics-we don’t just prevent allergies. We restore trust. This is what equity looks like: not just information, but access, dignity, and care.
It’s fascinating how the LEAP study’s effect size is misinterpreted as a universal protocol. The 80% reduction is conditional on strict adherence, baseline risk stratification, and controlled dosing-all of which are logistically unfeasible for 70% of the population. The real outcome? A medicalized parenting culture that pathologizes normal infant development. We’ve replaced instinct with algorithm, and now we’re surprised when parents feel overwhelmed.