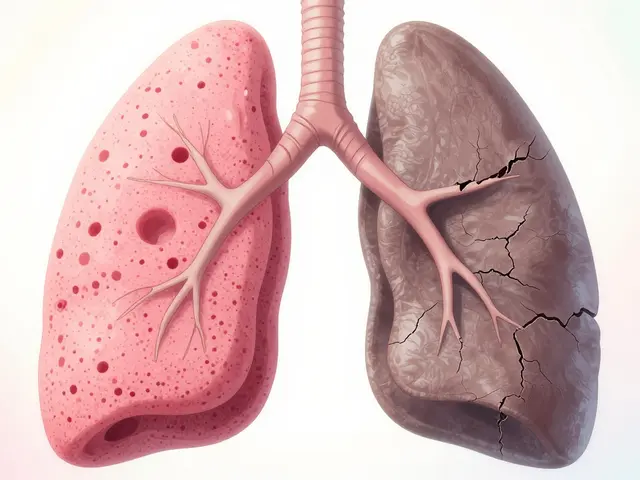
Imagine your lungs as a sponge, designed to be soft and flexible so they can easily soak up oxygen. Now, imagine that sponge slowly turning into a stiff, leather-like material. That is essentially what happens with Interstitial Lung Disease is an umbrella term for over 200 disorders that cause inflammation and progressive scarring (fibrosis) in the lung's interstitium-the delicate tissue surrounding the air sacs. When this tissue thickens, oxygen struggles to cross into your bloodstream, leaving you feeling winded even after a short walk to the mailbox. Because this scarring is typically irreversible, the goal isn't to "cure" the lungs, but to slow the damage and keep you active for as long as possible.
The Reality of Lung Scarring
In a healthy pair of lungs, the interstitium is incredibly thin-less than 0.1mm. But when Pulmonary Fibrosis occurs, this tissue can swell to 1-2mm or more. This isn't just a slight change; it's a total transformation of the lung's architecture. Your lungs lose their "compliance," meaning they can't expand fully when you breathe in.
Most people don't notice the signs right away. It usually starts as exertional dyspnea-that feeling of being out of breath during a brisk walk or climbing stairs. Over time, this can progress to shortness of breath even while sitting still. Along with the breathing struggle, about 78% of people deal with a persistent dry cough that just won't go away. You might also notice your fingertips widening, a condition known as clubbing, which happens in up to half of those with the more severe idiopathic forms of the disease.
Understanding the Different Types of ILD
Not all interstitial lung diseases are created equal. Some are caused by things we've been exposed to, while others appear for no apparent reason at all. Understanding which one you have is the only way to get the right treatment, as a drug that helps one person might do nothing for another.
The most common version is Idiopathic Pulmonary Fibrosis (or IPF), which makes up about 20-30% of cases. "Idiopathic" is just a medical way of saying "we don't know why this happened." IPF tends to be more aggressive, often affecting people over 75. On the other hand, some people develop ILD because of an autoimmune issue, like Rheumatoid Arthritis, which generally progresses more slowly.
| Subtype | Common Cause | Progression Speed | Typical Outcome |
|---|---|---|---|
| IPF | Unknown | Fast | Progressive decline in lung function |
| Connective Tissue ILD | Autoimmune (e.g., RA) | Moderate | Better 5-year survival rates (70-80%) |
| Sarcoidosis | Inflammatory | Variable | 60-70% may resolve spontaneously |
| Environmental/Asbestosis | Mineral fibers/Dust | Slow | Slow decline in forced vital capacity |
How Doctors Diagnose the Scarring
Getting a correct diagnosis is surprisingly tricky. Research shows that about 25-30% of patients are misdiagnosed initially, with many primary care doctors mistakenly attributing the shortness of breath to simple aging or asthma. This can lead to a frustrating gap of over 11 months between the first symptom and the correct answer.
The gold standard for seeing what's actually happening is a High-Resolution Computed Tomography (HRCT). Unlike a standard CT scan, an HRCT uses 1mm slices to catch the subtle "honeycombing" patterns of fibrosis that a regular X-ray might miss. To be sure, most hospitals use a multidisciplinary team-a pulmonologist, a radiologist, and a pathologist-to review the images together. They'll also run a Pulmonary Function Test (PFT) to measure your Forced Vital Capacity (FVC), which tells them exactly how much air your lungs can actually hold.
Treatment Options: Slowing the Slide
While we can't erase existing scars, we can put up a "roadblock" to stop new ones from forming. The focus has shifted from just treating symptoms to using Antifibrotic Therapy to slow the decline of lung function.
For those with IPF, the two heavy hitters are Nintedanib (Ofev) and Pirfenidone (Esbriet). These drugs can slow the drop in lung capacity by about 50% over a year. However, they come with a trade-off. Pirfenidone users often deal with skin sensitivity to sunlight (photosensitivity) and stomach issues. Nintedanib is similarly challenging for some. A newer option, zampilodib, was approved in 2023 and offers a different mechanism to further reduce the rate of lung decline.
Beyond Medication: Living with ILD
Drugs are only one part of the puzzle. To maintain a decent quality of life, most patients need a combination of supportive care and lifestyle adjustments.
- Pulmonary Rehabilitation: This is a supervised exercise and education program. It doesn't fix the lungs, but it teaches your muscles to use oxygen more efficiently. Many people see a significant jump in their "6-minute walk distance" after 8-12 weeks of rehab.
- Oxygen Therapy: When your resting oxygen saturation (SpO2) drops below 88%, supplemental oxygen becomes a necessity. It's not just about breathing; it's about protecting your heart from the strain of low oxygen.
- Energy Conservation: This involves learning how to pace your day. Simple changes, like sitting while dressing or using a shower chair, can save your precious energy for the things that matter most.
The Road Ahead: New Research
The future of ILD treatment is moving toward "personalized medicine." Instead of a one-size-fits-all drug, researchers are looking at genetic markers. For example, testing for the MUC5B promoter polymorphism can now help doctors predict if a patient's disease will progress rapidly. We're also seeing the rise of AI-assisted HRCT analysis, which can distinguish between ILD subtypes with 92% accuracy-beating the average human radiologist.
Current clinical trials are also exploring stem cell therapies and new tyrosine kinase inhibitors. The goal is to move beyond just slowing the disease and eventually find a way to repair the damage already done.
Can interstitial lung disease be cured?
Generally, no. Once lung tissue has turned into scar tissue (fibrosis), it cannot be reversed. However, treatments can slow the progression of the disease, manage symptoms, and prevent further damage, which significantly improves the quality of life.
What is the difference between IPF and other ILDs?
Idiopathic Pulmonary Fibrosis (IPF) is a specific type of ILD where the cause is unknown. Other ILDs have identifiable causes, such as autoimmune diseases (like rheumatoid arthritis), environmental exposures (like asbestos), or specific inflammatory conditions like sarcoidosis.
How quickly does ILD progress?
Progression varies wildly. IPF can be aggressive, with a median survival of 3-5 years without treatment. In contrast, connective tissue-related ILDs often progress much more slowly, and some forms, like sarcoidosis, may even resolve on their own.
When do I need to start using supplemental oxygen?
Medical guidelines generally recommend supplemental oxygen when your resting oxygen saturation (SpO2) levels drop below 88%. This helps prevent organ damage and reduces the strain on your heart.
Are the antifibrotic drugs worth the side effects?
For many, yes. Drugs like Nintedanib and Pirfenidone have been shown to reduce the decline of lung function (FVC) by about 50%. While side effects like nausea or photosensitivity are common, doctors can often manage these with dose adjustments.
Next Steps and Troubleshooting
If you or a loved one are experiencing a persistent dry cough and shortness of breath, don't assume it's just a sign of getting older. Start by requesting a full pulmonary function test and a referral to a pulmonologist. If you've already been diagnosed, the next critical step is finding a multidisciplinary ILD clinic; these centers provide a coordinated approach between radiologists and pathologists that community hospitals often lack.
For those currently on antifibrotics, keep a detailed log of your side effects. If you're experiencing severe GI distress or skin rashes, don't stop the medication abruptly. Instead, ask your doctor about "dose titration"-a method of slowly adjusting the amount of drug to find a balance between efficacy and tolerability.